August 8, 2013:
In 1963 when Kenneth Arrow wrote his seminal piece on ‘Uncertainty &Welfare Economics of Medical Care’, it not just stirred the scholarly debate on the economics of health care but it continues to form the basis of the theory taught even in today’s health economics class.
But is this now changing? Arrow’s theory was based on the premise that unlike other goods and commodities, when it comes to medical goods and services there exists information asymmetry between consumers of health care and the suppliers— in this case the physicians and health care providers. As a result, physicians will always have an advantage in pricing as consumer cannot completely know as much about their own health needs as would a doctor.
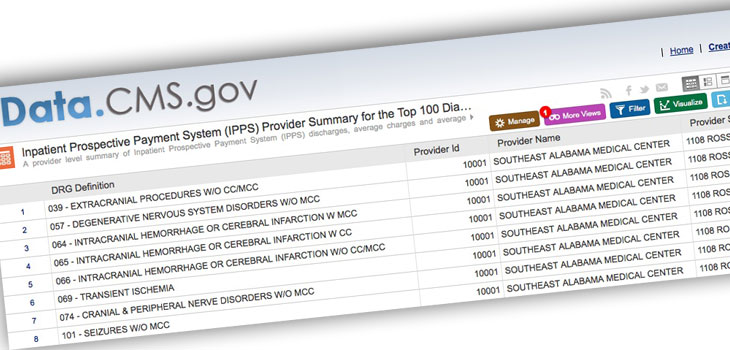
Today thanks to information technology that this asymmetry of information is narrowing in certain countries like the US. In the US, the government has released data for the first time on variation in hospital prices for the top 100 diagnosis-related groups for Medicare patients. Diagnosis-related Groups is a classification system to group patients based on certain diseases and procedures incurred to treat them, thereby making it possible to compare costs for the same disease. Since Medicare is a program funded by the US department of health and human services for its citizens above 65 and disabled, the government reimburses to the hospitals a part of the cost incurred by them for conducting certain procedures, and the remainder of the amount is billed to the patient or to the insurance companies. The way the reimbursement is calculated to the hospitals is based on a variety of factors such as its labor costs and other input costs based on a hospitals location in a certain metropolitan statistical area and its characteristics. Hospital characteristics that drive variation in prices for the same surgical procedure but in different hospital setting depend on whether the hospital is a teaching hospital or a non-teaching entity, the share of the population it treats with no insurance, the share of the population it treats which have a low income and thus participate in certain safety net programs, and on ownership factors such as whether it is a government, private, not-for-profit organization among others. The government then computes the reimbursement for all the hospitals based on some of these characteristics. Thus consumers, policy makers, and employers can compare not only what a hospital charges them for a specific disease but also can compare it to benchmark average at a state and national level. And a prudent consumer can accordingly decide his or her options to avail care, given he has the knowledge about the standardized disease code or the procedure for which he or she will be operated.
Now is this relevant in the Indian context? Importantly, can it be possible for the government to regulate the hospitals and the insurance companies in publishing this kind of data on hospital costs associated with the same surgical procedure? Researchers at the Public Health Foundation, Chatterjee, Sushmita and Laxminarayan, Ramanan recently conducted a similar study to detect variation in hospital costs with a sample of 5 hospitals with varying characteristics such as private, district level or tertiary care among others. And any such study that could cover more hospitals by a researcher will have limitations because only the government can have the wherewithal to furnish large scale national data of this kind.
While in a country where out of pocket expenses constitute a fairly high share of overall health spending in comparison to other countries and an increased share of tertiary care and multi-speciality hospitals are being concentrated in urban settings, this kind of information can certain help consumers within the same geographical area to make better informed decisions or those travelling from smaller cities as well. At the same time increased transparency in hospital prices could also possibly benefit the medical tourism industry clients who currently can view the nearest hotels but not compare the prices of another hospital in its proximity.
But unlike in the US where the government provides subsidies even to the private hospitals depending on their teaching/non-teaching status, treatment of low-income population or without any form of health insurance, this is not the case in India. This also makes hospitals less accountable to the government and in complying with the latter to provide such data.
When it comes to making public policy decisions by the government, there are always two parties that favor the same regulation for completely different reasons —the Baptists and the bootleggers. The Baptist will favor a regulation for ethical reasons; the bootlegger will because increased regulation would benefit his own industry. Extending the same analogy in the Indian health care setting, the Baptist would certainly be the consumer and non-profit organization advocates who will benefit and would favor such a regulation even on ethical grounds. Who will be the bootlegger? Will it be the medical tourism industry or the health insurance companies?